
Beginning this year, the Medicare Stars adherence measures are risk-adjusted based on four sociodemographic status (SDS) risk factors (age, sex, LIS status, and disability). This adjustment is a substantive change to the measures, which results in a one-year change in their weighting from a triple weighted measure to a single weight.
Despite the significance of this change, Medicare has released minimal information on how the risk-adjusted adherence measures will be calculated and what impact this will have on a plan sponsor’s Star Ratings.
Translating What We Know Right Now
Within the final release of the 2024 Acumen reports, Medicare finally gave plan sponsors their first glimpse of the risk adjusted rates. The Acumen package included the technical specification guide that showed the SDS risk-adjustment equation and the 2024 results from the multivariate random effects logistic regression model. Within the technical specifications, CMS revealed for the first time the equation that will be used to calculate a plan sponsors risk-adjusted adherence rate.
The equation from the technical specification guide is:
Risk Adjusted Adherence Rate = (Unadjusted Rate/Predicted Rate) x Contract Type Unadjusted Rate
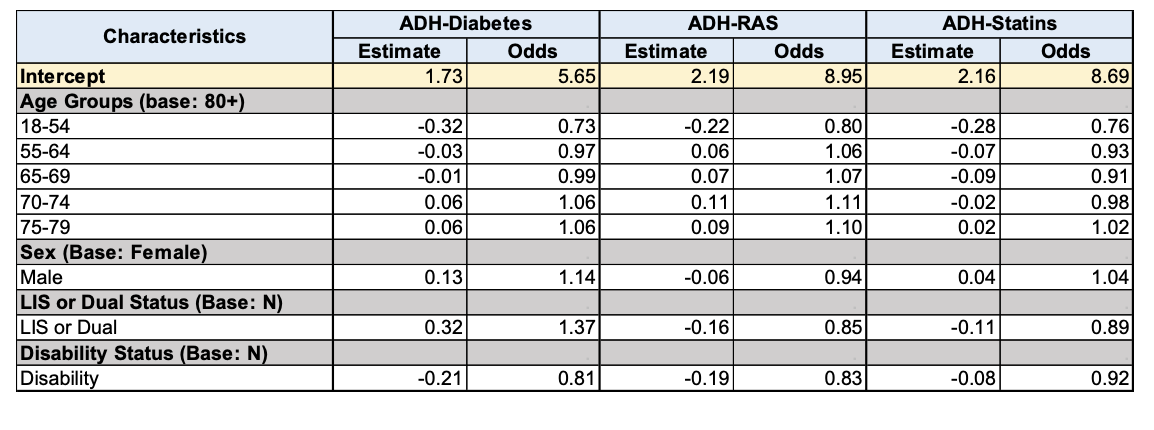
The Acumen data shows plan sponsors their risk adjusted rate, unadjusted rate, and contract type unadjusted rate. What it does not provide is the plan sponsors predicted rate or how it is calculated. Instead, the Acumen report displays the model results for each risk factor, by measure used in the predicated rate calculation as shown in the table below.
2024 Multivariate Random Effects Logistic Model Regression Model Results
Even if the plan sponsor were to give this information to their actuaries or statisticians, it would not be helpful during the measurement year, sinceMedicare intends to release this information in the final Acumen report the following year. But when you view this initial data release alongside the stratified adherence rates in the Acumen report, they do point to which populations will have the largest impact on the risk adjusted adherence rates.
The Numbers Tell a Story
Looking at the data, there are three main drivers for the risk-adjusted adherence measures.
- Age 18-54
- Disability
- LIS/DE status
While Medicare reports adherence rates individually for each of these categories, these 3 demographics point to a part of the membership that disproportionately underperforms in medication adherence:The younger member that qualified for Medicare services due to a disability.
Here’s what matters:
- One in eight Medicare beneficiaries qualifies through disability rather than age. That's 7.7 million people under 65 enrolled in Medicare. They account for more than 17% of all Medicare spending.
- Their adherence rates lag significantly. Disabled beneficiaries perform3% lower across all three medication adherence measures compared to non-disabled beneficiaries. They also underperform dual-eligible and LIS populations by 1-3% depending on the measure.
This gap represents your biggest opportunity under SDS risk adjustment.
Why This Population Is Different and More Challenging
Disabled beneficiaries face unique barriers that traditional adherence programs miss. Understanding these differences is critical. Forty-two percent of disabled Medicare beneficiaries qualified due to cognitive impairment which is their primary diagnosis rather than a physical disability. This fact fundamentally changes how they interact with the healthcare system.
These members may also have lower incomes and education levels than traditional Medicare enrollees. They report lower overall health scores. They experience worse access to care and more cost concerns. They have lower satisfaction with their care overall.
What matters most is that this population self-reports having more difficulty navigating their healthcare experience. They struggle to be their best advocates in a fragmented healthcare ecosystem. They are younger and facing complex healthcare needs at a stage of life when their peers aren't dealing with chronic conditions.
The healthcare system wasn't designed for them. Benefits aren't structured for easy access to the care they need. Standard outreach doesn't account for cognitive barriers. Traditional care coordination misses the depth of support required.
Physical disabilities create one set of access challenges. Cognitive and behavioral impairments create entirely different ones. Yet most plans use the same playbook for all disabled members. This issue explains the persistent adherence gap—and why closing it requires specialized approaches.
What SDS Risk Adjustment Changes Now
SDS risk adjustment doesn't just recalibrate your scores. It forces a strategic question. Are you equipped to serve your highest-risk members effectively?
Plans serving significant disabled populations now have a measurement framework that accounts for this complexity. Your performance will be compared more fairly. But that only matters if you build the right infrastructure now.
Remember the timeline. SDS-adjusted measures enter Star Ratings in measurement year 2026 at 1x weighting. Then they return to 3x weighting in measurement year 2027. Strong performance in 2026 sets you up for success when triple weighting returns.
Where to Focus Your Efforts
Health plan leaders need systems that identify at-risk disabled members in real time. Organizations need care teams trained to address cognitive, physical, and behavioral barriers. This work demands personalized outreach that goes beyond standard education and reminders.
The first step is a sophisticated data analysis to understand your specific disabled population. It requires care coordination to resolve transportation, appointment, and billing issues. Economic challenges like housing and food insecurity may apply. But what are the greatest challenges that compromise access to healthcare for those with physical, cognitive, or behavioral impairment?
Significant care coordination is required to resolve issues and improve outcomes for this group. Most importantly, it requires starting now – and being open to asking for help.
Are you interested in closing the disability gap in your adherence performance? Learn more at actualmeds.com/solutions#adherence-stars or contact our team today.


